Cancer, Sex, and the Male Body
When someone is diagnosed with cancer, they may wonder how ‘normal’ life can and will be if they need to go through surgery or treatment, or as they adjust to living as a survivor. Many times a person with cancer wonders how the diagnosis and treatment might affect their sex life.
Information about sexuality is important for people with cancer
Sex, sexuality, and intimacy are just as important for people with cancer as they are for people who don’t have cancer. In fact, sexuality and intimacy have been shown to help people face cancer by helping them deal with feelings of distress, and when going through treatment. But, the reality is that a person's sex organs, sexual desire (sex drive or libido), sexual function, well-being, and body image can be affected by having cancer and cancer treatment. How a person shows sexuality can also be affected. Read more in How Cancer and Cancer Treatment Can Affect Sexuality.
The information here is for adult males who want to learn more about how cancer and cancer treatment can affect their sex life. We cannot answer every question, but we’ll try to give you enough information for you and your partner to have open, honest talks about intimacy and sex. We’ll also share some ideas to help you talk with your doctor and your cancer care team.
If you are gay, bisexual, transgender (LGBT) or gender non-conforming, you may have needs that are not addressed here. It's very important to talk to your cancer care team and give them information about your sexual orientation and gender identity, including what sex you were at birth, how you describe yourself now, any procedures you’ve had done, or hormone treatments you may have taken or are taking.
The 1st step: Good communication
The first step is to bring up the topic of sex with your partner and cancer care team. It’s very important to talk about what to expect, and continue to talk about what's changing or has changed in your sexual life as you go through procedures, treatments, and follow-up care. Don't assume your doctor or nurse will ask you about any concerns you have about sexuality. You might have to start the conversation yourself. Many studies have found that doctors, nurses, and other members of a health care team don’t always ask about sexuality, sexual orientation, or gender identity during check-ups and treatment visits. Because of this, patients might not get enough information, support, or resources to help them deal with their feelings and sexual problems.
You probably have certain questions and things you're wondering about. Here are some questions you can use to jump start talks with your cancer care team about having sex during and after treatment:
- How might treatment affect my sex life?
- Is it safe to have sex now? If not, when will it be OK to have sex?
- Are there any types of sex I should avoid?
- Do I need to use birth control?
- Does my partner need to use birth control while I'm on treatment? What about afterward?
- Can my body fluids pass on medications or treatments (such as radiation) to my partner?
- What safety measures do I need to take, and for how long?
The 2nd step: Understanding how male body parts work
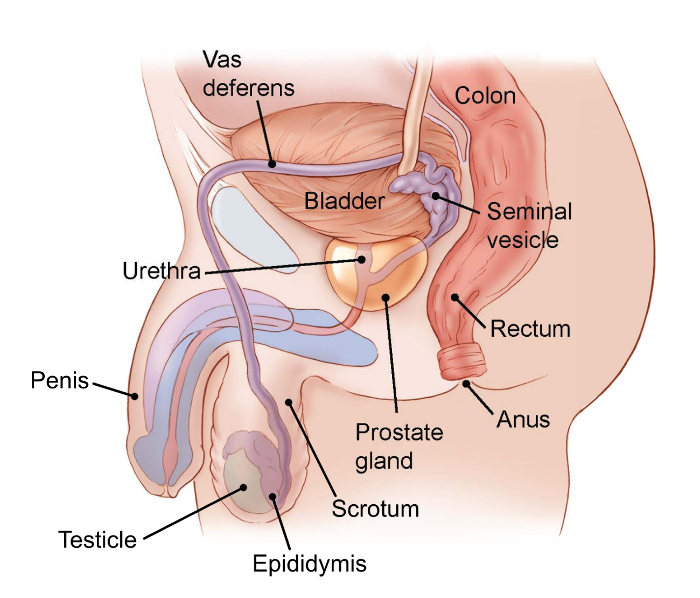
A man’s genitals and sex organs are in the pelvis (the lower part of the belly) and in the front of the body between the legs. Here are some of the organs in or near the pelvis, including sex organs and other nearby organs. Cancer of any of these organs or cancer treatment in this area can affect your sex life:
- Scrotum – the sac or pouch that hangs below the penis and holds the testicles and epididymis.
- Testicles (testes) – the 2 oval organs inside the scrotum that produce a steady supply of hormones, mostly testosterone. They also make millions of sperm each day.
- Epididymis – a very thin, long coiled tube that sits on top of and behind each testicle. The sperm must travel through the epididymis to mature.
- Vas deferens – the tubes on either side of the body that mature sperm must travel through just before ejaculation. Each tube carries sperm from an epididymis into the body toward the prostate gland.
- Prostate gland – a walnut-shaped gland that sits in front of the rectum and below the bladder. The prostate surrounds the urethra. This gland is where the sperm is mixed with fluids from the prostate and the seminal vesicles. This whitish, protein-rich fluid helps to support and nourish the sperm so that they can live for some time after ejaculation.
- Seminal vesicles – pouches attached to the vas deferens that make part of the fluid that helps support the sperm. During orgasm this mixture of fluid and sperm, called semen, moves through the urethra and out of the tip of the penis.
- Urethra – the tube that goes through the penis to carry both urine from the bladder and semen out of the body.
- Penis – the male organ used for sex. It’s filled with spongy tissues that fill with blood to produce an erection when a man is aroused.
- Bladder – the hollow, balloon-like organ that holds urine.
- Rectum – the bottom end of the intestines that connects to the outside of the body.
The drawing below shows a side view of the male sex organs and nearby structures.
Understanding the role of testosterone
Testosterone is the main male hormone. It causes the reproductive organs to develop, and promotes erections and sexual behavior. Testosterone also causes secondary sexual characteristics at puberty, such as a deeper voice and hair growth on the body and face. The testicles make most of this hormone. The adrenal glands, which sit on top of the kidneys, also make small amounts of testosterone in both men and women.
Men’s hormone levels vary widely, but most men have more testosterone in the bloodstream than they need. A man with a low level of testosterone may have trouble getting or keeping erections and may lose his desire for sex. Testosterone levels tend to decrease as a man ages.
The normal pattern of arousal and erection
An erection begins when the brain sends a signal down the spinal cord and through the nerves that sweep down into the pelvis. Some of the important nerves that produce an erection run close to the rectum (the last part of the large intestine) and along both sides of the prostate.
When this signal is received, the spongy tissue inside the shaft of the penis relaxes and the arteries (blood vessels) that carry blood into the penis expand. As the walls of these blood vessels stretch, blood quickly fills 2 spongy tubes of tissue inside the shaft of the penis. The veins in the penis, which normally drain blood out of the penis, squeeze shut so that more blood stays inside. This causes a great increase in blood pressure inside the penis, which produces a firm erection.
The nerves that allow a man to feel pleasure when the penis is touched run in a different path from the nerves that control blood flow and produce an erection. So, even if nerve damage or blocked blood vessels keep a man from getting erections, he can almost always feel pleasure from being touched. He can also still reach orgasm.
A third set of nerves, which run higher up in a man’s body, control the ejaculation of semen.
How male orgasm happens
A man’s orgasm has 2 stages:
The first stage is called emission. This is when the prostate, seminal vesicles, and vas deferens contract. During emission, the semen is deposited near the top of the urethra, so that it’s ready to be pushed out (ejaculated). At this time, a small valve at the top of the tube shuts to keep the semen from going upward and into the bladder. A man feels emission as “the point of no return,” when he knows he’s about to have an orgasm. Emission is controlled by the sympathetic or involuntary nervous system.
Ejaculation is the second stage of orgasm. It’s controlled by the same nerves that carry pleasure signals when the genital area is caressed. Those nerves cause the muscles around the base of the penis to squeeze in rhythm, pushing the semen through the urethra and out of the penis. At the same time, messages of pleasure are sent to the man’s brain. This sensation is known as orgasm or climax.
The 3rd step: Keep talking and work together to manage problems
Learn as much as you can about the possible effects your cancer treatment may have on your sex life. Talk with your doctor, nurse, or any other member of your cancer care team. When you know what to expect, you can plan how you might handle those issues.
Keep in mind that, no matter what kind of cancer treatment you get, most men can still feel pleasure from touching. Few cancer treatments (other than those affecting some areas of the brain or spinal cord) damage the nerves and muscles involved in feeling pleasure from touch and reaching orgasm. For example, some types of treatment can damage a man’s ability to have erections. But most men who can’t have erections or produce semen can still have the feeling of orgasm with the right kind of touching.
Try to keep an open mind about ways to feel sexual pleasure. Some couples have a narrow view of what normal sex is. If both partners can’t reach orgasm through or during penetration, some may feel disappointed. But during and after cancer treatment, there may be times when the kind of sex you like best is not possible. Those times can be a chance to learn new ways to give and receive sexual pleasure. You and your partner can help each other reach orgasm through touching and stroking. At times, just cuddling can be pleasurable. You can also continue to enjoy touching yourself. Do not stop sexual pleasure just because your usual routine has been changed.
Try to have clear, 2-way talks about sex with your partner and with your doctor. If you’re too embarrassed to ask your doctor whether sexual activity is OK, you may never find out. Talk to your doctor and tell your partner what you learn. Good communication is the key to adjusting your sexual routine when cancer changes your body. If you feel weak or tired and want your partner to take a more active role in touching you, say so. If some part of your body is tender or sore, you can guide your partner’s touches to avoid pain. Keep in mind that if one partner has a sex problem, it affects both of you.
Boost your confidence. Remind yourself about your good qualities. Eating right and exercising can help keep your body strong and your spirits up. Talk to your doctor or cancer care team about the type of exercise you’re planning before you start, or ask to be referred to a physical therapist. Find something that helps you relax – movies, hobbies, or getting outdoors. Practice relaxation techniques, and get professional help if you think you are depressed or struggling.
- Written by
- References
The American Cancer Society medical and editorial content team
Our team is made up of doctors and oncology certified nurses with deep knowledge of cancer care as well as editors and translators with extensive experience in medical writing.
American Association of Clinical Endocrinologists. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for the Evaluation and Treatment of Male Sexual Dysfunction: A couple’s problem – 2003. Update Endocr Pract. 2003;9(No. 1). Accessed at https://www.aace.com/sites/default/files/2019-06/sexdysguid.pdf on January 31, 2020.
Carter et al. Interventions to address sexual problems in people with cancer: American Society of Clinical Oncology clinical practice guideline adaptation of Cancer Care Ontario guideline. Journal of Clinical Oncology. 2018;36(5):492-513.
Katz A. Breaking the Silence on Cancer and Sexuality: A Handbook for Healthcare Providers. 2nd ed. Pittsburgh, PA: Oncology Nursing Society.; 2018.
Katz, A. Man Cancer Sex. Pittsburgh: Hygeia Media, 2010.
Khera M, Snyder PJ, Martin KA. Treatment of male sexual dysfunction. UpToDate. 2019. Accessed at https://www.uptodate.com/contents/treatment-of-male-sexual-dysfunction on January 31, 2020.
Moment A. Sexuality, intimacy, and cancer. In Abrahm JL, ed. A Physician’s Guide to Pain and Symptom Management in Cancer Patients. Baltimore, MD: Johns Hopkins University Press; 2014:390-426.
National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology: Survivorship [Version 2.2019]. Accessed at https://www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf on January 31, 2020.
Nishimoto PW, Mark DD. Sexuality and reproductive issues. In Brown CG, ed. A Guide to Oncology Symptom Management. 2nd ed. Pittsburgh, PA: Oncology Nursing Society; 2015:551-597.
Zhou ES, Bober SL. Sexual problems. In DeVita VT, Lawrence TS, Rosenberg SA, eds. DeVita, Hellman, and Rosenberg’s Cancer: Principles and Practice of Oncology. 11th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2019:2220-2229.
Last Revised: February 1, 2020
American Cancer Society medical information is copyrighted material. For reprint requests, please see our Content Usage Policy.
American Cancer Society Emails
Sign up to stay up-to-date with news, valuable information, and ways to get involved with the American Cancer Society.

